
What is posterior cervical foraminotomy?
Posterior = back of your neck
Cervical = the area at the top of your spine aka your neck
Foramen = an opening in your spine that the spinal nerves travel to exit the spinal cord
“otomy” = means to make an opening. In this case, to make more room/opening for the spinal nerves.
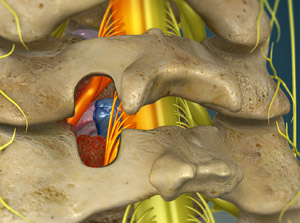
Posterior Cervical Foraminotomy = a procedure done through the back of your neck to make more room for the spinal nerves.
Approach
The surgery is done by making a small incision on the back of your neck.
The Procedure
Anesthesia & Induction
- Your anesthesiologist will talk to you about the specifics of his/her plan for the procedure. You will find out what medications and what type of anesthesia will be used to keep you pain free and comfortable throughout the operation.
- In general, most patients will undergo general anesthesia during spine procedures meaning you will be asleep and wont remember or feel any pain during the procedure itself. Patients may have pain upon waking up from anesthesia, but this will be managed with intravenous and oral pain medications.
- After a breathing tube is placed and you are fully asleep, you will be positioned on the operating room table.
- Surgery will not begin until you are asleep and given pain medications so that you don’t feel any pain during the procedure.
Incision
- After localizing the correct level with x-ray, a skin incision is made on the posterior aspect of your neck.
- The posterior muscles in your neck are carefully moved off of the bone and held apart with the use of special tools, called retractors.
Performing the Decompression
- Before removing the diseased disc that is pressing on your spinal nerve, Dr. Webb will confirm that he is operating at the correct level by taking an x-ray while you are asleep.
- When the level is confirmed, Dr. Webb will then begin the decompression (removing the areas of compression from your spinal cord) portion of the procedure by carefully remove the disc that is pressing on your spinal cord/nerves with the use of special instruments and tools.
- At times, Dr. Webb will use a microscope during surgery to complete the operation. This allows him to see small structures, such as your nerves, with finer detail.
- With the diseased disc removed, any additional surrounding structures which may be pressing on your spinal cord, such as bone spurs and/or excess ligaments, will be removed.
- Webb will then ensure that your spinal cord and nerves are free from compression.
Closure
- The retractors that held the muscles apart, so Dr. Webb can complete the decompression, will now be removed. The muscles that were moved will then fall back into their original place.
- Webb uses absorbable sutures to close your wound. These sutures do not typically need to be removed and will absorb on their own.
- Sometimes, a special tube called a drain will be used. This is to collect any blood or fluids that can collect after surgery. This drain will be removed before you leave the hospital, usually the next day after surgery.
What to expect after Surgery
After surgery you will be transferred to the recovery room, also called the PACU (post anesthesia care unit). After you have awaken from the anesthesia, you will then be transferred to your hospital room. This is typically when your family members can visit you.
Either the same day or the following morning after surgery, a physical and/or occupational therapist will begin your therapy. During your hospital stay, you will be given medications to help with pain and IV antibiotics to minimize the risk of infection. Most patients spend 1-2 nights in the hospital and are discharged home after:
- You are tolerating a diet
- Your pain is controlled
- After you have worked with and passed physical therapy.
Walking after surgery is highly encouraged, even the same day of surgery!
Frequently Asked Questions
What kind of recovery can you expect after surgery?
Recovery from posterior cervical foraminotomy surgery can take 4-6 weeks, but patients continue to heal for up to a year after surgery.
When can I return to work and/or activities?
Walking is highly encouraged, immediately after surgery and throughout your post operative period. Most patients can return to a light desk job or household activities by 2-3 weeks after surgery.
When will my neck or arm pain go away?
If you can imagine putting your elbow on a hard surface for a long time, what happens? Your fingers start to go to sleep. Why? Because the nerves to these fingers is compressed, is asleep, and is irritable. Once you realize this, you pick up your elbow (to remove the pressure off of the nerve) and shake your fingers until they wake up. This is a similar concept in spine surgery where depending on how long your nerves and spinal cord have been compressed, will determine how long it takes for the nerve to wake up after the surgery. If you have had compression of your nerves and spinal cord for months to years, then it may take some time before the nerve recovers and wakes up (if it recovers at all). Most patients, however wake up from surgery with arm pain relief meaning that the debilitating arm pain they had before surgery has went away, but may have some neck pain and spasms from the surgical incision itself. This pain will be controlled with oral/IV pain medications and antispasm medications throughout your hospital stay.
What complications should I be aware of?
Inadequate relief of symptoms
- Webb is very particular about making sure we target the right level of your spine that may be causing your symptoms.
- Inadequate relief of symptoms after surgery could be due to a number of things including: multiple levels that are degenerated or worn out that will not be addressed in surgery, surgery done on the wrong level, or advanced and severe spinal cord compression that may be irreversible.
- Injections are confirmatory and are very predictive of how well you will do with surgery. These spinal injections, usually done before surgery in the conservative treatment period, are essential in determining which level of your spine is the cause of your symptoms.
- Just because you have multiple degenerated areas of your spine according to your imaging studies (MRI, X-ray, etc.), does not mean every level needs an operation. Dr. Webb believes in symptom specific surgery.
Dural tear
- The dura is the outer layer of the spinal cord. Sometimes, this layer can be especially thin in certain patients and very friable. During surgery, if there is a small tear in this layer, Dr. Webb will attempt to repair it. This is a not a very common complication, but definitely one that needs to be known.
- Sometimes after a dural tear is repaired, Dr. Webb may ask that you to sit upright for 24 hours after surgery. This is done to give the repair time to heal and to ensure his repair does not come apart.
- Fortunately, multiple studies have shown that having a dural tear repair does not affect your outcome from surgery.
Infection
- Very low risk (<1%) but this risk is increased if you are overweight, immunosuppressed, on chronic steroids, or diabetic.
- Antibiotics will be given before surgery starts and also given for 24 hours after surgery while you are in the hospital to decrease the risk of infection.
Bleeding
- Very low risk, but increased if you are taking blood thinners, fish oil, herbal medications or have a clotting disorder.
- Sometimes, a special tube called a drain will be placed during surgery. This tube is to collect any blood or fluids that can collect after surgery. This drain will be removed before you leave the hospital, usually the next day after surgery.
Spinal cord or Nerve damage
- Low risk
- A neuromonitoring technician is a professional trained in the monitoring of your nerves and spinal cord.
- This person (along with a Neurologist) is part of the team that will be taking care of you during surgery and will help Dr. Webb monitor your nerves and spinal cord throughout the procedure.
- You will be able to meet this person the morning of surgery and ask any questions about their role in your care.
- Generally, after you are asleep from anesthesia, this technician will place small wires on your legs and arms so that the nerves and spinal cord and be monitored during surgery.
Reoperation
- Some patients who do not get full relief of their symptoms may require additional surgery, such as a fusion, to relieve their symptoms.